A large number of measles cases were reported from Riyadh region, particularly among school age children in May 2004, immediately after the measles vaccination campaign for primary school students. It was feared that this increase may be related to the vaccination campaign.
As a first step, a descriptive study of all the measles cases reported in Riyadh during 2004 was conducted, by reviewing the records and interviewing patients. This was followed by a case-control study to identify the associated risk factors. A case was defined as any person living in catchment area, who presented during 2004 with generalized maculopapular rash lasting 3 or more days, elevated temperature 38.3°C or higher, with cough, coryza or conjunctivitis and confirmed by positive serologic test for IgM. A control was defined as any person who never had symptoms suggestive of measles during 2004 and lived in the catchment area of the same Primary health care center from where the case was reported, selected from the family files of the primary health centre.
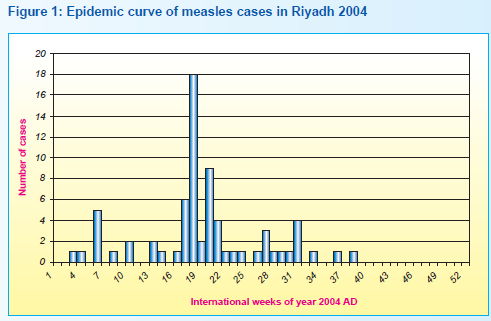
During the years 2000, 2001, 2002, 2003 the total number of reported measles cases was 95, 18, 56 and 78 respectively; compared to 204 cases in 2004. The mean number of cases for earlier years was 50.67 (95% CI 16.3-85.0), the 204 cases were clearly excess of the +2SE limit for outbreak definition. The maximum number of cases were reported in May 2004, gradually falling afterwards and disappearing by October (Figure 1).
A total of 70 cases were traceable and included in the study; 87.1% were Saudis; 34.3% were under 5 years of age, 40% were 6€“10 years old, and 25.7% were over 10; 30% lived in Al-mansourah, 17.1% in Oraija and the rest were scattered over the city. Most of the cases were females (65.7%) and 58.6% were students. Out of 41 students, 17 (42.5%) were from the same girls€™ school. All of the cases presented with history of fever and skin rash, 64.3% with cough and coryza and 57.1% with conjunctivitis. Thirty percent of the cases developed chest infection, 20% diarrhea, 8.6% ear problem and 5.7% convulsions. All cases were serologically positive for measles. About 24% were admitted into hospital, and no deaths occurred among them.
Sixty six controls were selected. More than 90% of both cases and controls had history of measles vaccination, while there was a statistically non-significant higher proportion vaccinated among the controls (91.3% & 96.6% respectively; OR 0.37; 95% CI 0.07-1.90). There was no association of vaccination during 2004 and disease status. However, cases had a significantly higher history of contact with a measles case as compared to the controls (64.5% & 8.3% respectively; OR 20.0; 95% CI 6.98-57.33).
Editorial note:
Before introduction of routine measles vaccination in 1983, the incidence of measles infection in Saudi Arabia was alarmingly high. In this study, a large proportion of cases were in the 5-10 year age group, which is consistent with previous studies.[1,2]
The shift in age distribution of cases towards older children is one of the major effects of immunization programs on the epidemiology of the disease due to lowering the exposure rate in the community.[3]
In 1983, to increase vaccination coverage rates, the measles vaccine was made a requirement for obtaining the birth certificate. Consequently, coverage increased from 8% in 1980 to 80% in 1984, and to >90% in 1990. Although a remarkable decrease in measles incidence ensued in general, the overall impact of immunization remained unsatisfactory. A substantial number of cases continued to occur in children aged under 9 months, and infection also shifted to older age groups, with a large proportion of cases appearing among previously vaccinated children.[2,4] In this study, over 90% of measles occurred among immunized individuals. The large number of cases occurring among immunized individuals is related to the level of coverage achieved.[3]
The role of vaccination failure is often difficult to assess. However, the accepted failure rate (derived from serological result) is in the range of 2% to 10%.[5] It was noted that there was a measles campaign during the time of discovering the increasing number of cases. Although we tried to look for any relationship of cases to a specific vaccine but were not able to do so due to lack of information in the vaccination records of the Primary Health Care Centers, which do not record the batch numbers and the countries of origin of the vaccine. Further, there was no evidence to correlate the measles cases with the measles campaign held in 2004.
References
- Kamel MI et al. Comparison of some epidemiological characteristics of vaccinated and unvaccinated measles cases in Saudi Arabia. Alex J Ped 1989,3(4): 5452.
- Tayil SE, El-Shazly M K, El-Amrawy SM, Ghouneim FM, Abou Khatwa SA, Masoud GM. Sero-epidemiological study of measles after 15 years of compulsory vaccination in Alexandria, Egypt. East Med Hlth J 1998; 4(3): 437-47.
- Global programme for vaccines and immunization. Immunization policy. Geneva, WHO, 1995 (WHO/EPI/ GEN/95.3).
- Albanamy A. Measles vaccine failure. Annals of Saudi Medicine 1991. 11: 311-4
- Wilkins J, Wehle PF. Evidence for reinstatement of infant 12 to 14 months of age into routine measles immunization programs. Am J Dis Child 1978; 132:164-6.