Eight years ago, Saudi Arabia started National Tuberculosis Control Program (NTCP) activities according to guidelines of the eighth and ninth reports of the World Health Organization expert committee on tuberculosis (TB). The objectives of the program are to reduce the incidence of TB and eliminate it as a health problem; to reduce human suffering (morbidity and mortality), and to assess the extent and efficiency of existing health facilities for TB control.
The public health approach for TB prevention and control in Saudi Arabia has two parts:
- Identify and treat persons with TB disease to cure their illness and prevent further transmission
- Identify and treat persons with TB infection (tuberculin-positive) to prevent development of the disease.
The NTCP is a country-wide program adapted to the needs of the population and integrated into the activities of primary health care centers (PHCCs). It is executed through early case detection (smear-positive) and adequate chemotherapy with follow-up and defaulter retrieving, chemoprophylaxis for high-risk groups, BCG immunization for children and health education with community participation.
At the central level, the Chest Disease Section of the Ministry of Health's Infectious and Parasitic Disease Department cooperates with the NTCP committee in planning, coordination of supervision, training, surveillance, evaluation, research and cooperation with the World Health Organization and the International Union Against Tuberculosis and Lung Diseases. At the regional level, the Ministry of Health's Directorate for General Health Affairs and the NTCP coordinator work together on supervision, training, coordination and collection of statistical data. Finally, at the local level, the program is actually implemented by the PHCCs, chest units, chest hospitals and the district directorate supervisor. This entails case finding, treatment, case holding, on-the-job training in reporting and recording, and health education.
In February 1992, the deputy minister for preventive medicine established and became chairman of an advisory committee for the NTCP. A series of introductory training courses is being conducted in all regions; since the start of the courses in 1992, 16 of 19 regions have been covered. Trainees include physicians, nurses, social workers and laboratory technicians.
Surveillance results: In 1993, 2,106 new cases of pulmonary TB were reported. Of these, 954 were Saudi (45.3%) and 1,152 were non-Saudi (54.7%). Nationalities of the non-Saudis were not available. Males accounted for 77.9% of the non-Saudis. The greatest number of cases overall were found in the 15-44 age group (1,385; 65.7%), followed by 45 years (632; 29.5%). In the same year, 280 cases of non-pulmonary TB were reported: Saudis 151 (53.9%) and non-Saudis 129 (46.1%).
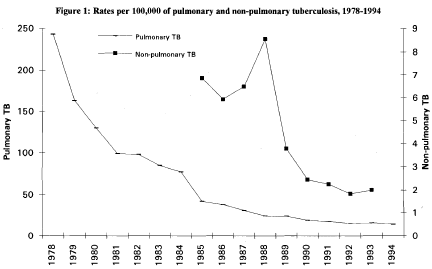
The number of cases increased in both Jeddah (482; 22.8%) and Gizan (279; 13.2%) regions in 1993. Overall, however, the incidence of TB has been decreasing since 1978, when the rate was 243/100,000 population (Figure 1). In 1994 it was 13.9/100,000.
Editorial note:
TB remains one of the top priorities for preventive action in developing counties, where over 85% of the world's TB now occurs. Each year about 10 million people in poorer countries are thought to develop TB, and at least 3 million die of the disease.[1] The incidence of pulmonary TB in the Kingdom has steadily decreased from 1978 until 1992 at a rate of 15% annually, and the line graph resembles one of the TB incidence in developed countries in the beginning of this century. This decrease can be attributed to improved case finding, diagnostic tools and management, an active vaccination program, and improvement in the socioeconomic status of the population.
In 1993 the incidence increased by 4.8%, which can be attributed to heightened awareness of TB among health personnel, who received 11 intensive courses in TB case-finding and control in 1993. TB in the Kingdom comes from expatriates from high-prevalence countries; in addition to being a source of infection, they carry a multi-resistant tubercule, so all new arrivals in the Kingdom need to pass a screening test for TB (PPD test and chest X-ray) for issuance of a valid residency permit. The most productive population age group (15-44) has the highest infection rate in the Kingdom; this group also has the highest death rate in developing countries.[2] The economic cost of TB in terms of lost production alone must be greater than that of a disease that exclusively affects children or the elderly.
References
- Fox E. Tuberculosis. In: Strickland GT. Hunter's tropical medicine (7th ed.). Philadelphia: WB Saunders 1991: 458483.
- Murray C, Styblo K, Rouillon A. Tuberculosis. In: Jamison D, Mosley W, Measham A, Bobadilla J (eds.). Disease control priorities in developing countries. Oxford: Oxford University Press 1993: 233-259.